
Translate this page into:
Severe acute respiratory syndrome corona virus-2 disease and the community pharmacist: Practical lessons from the trenches

*Corresponding author: Olugbade O. Bolanle, Merciland Farmacie, Southgate, Michigan, United States. tosh@mercilandfarmacie.com
-
Received: ,
Accepted: ,
How to cite this article: Bolanle OO. Severe acute respiratory syndrome corona virus-2 disease and the community pharmacist: Practical lessons from the trenches. Am J Biopharm Pharm Sci 2022;2:4.
Abstract
Severe acute respiratory syndrome corona virus-2 (SARS-CoV-2) disease represented a systemic stress test of sorts on a global scale both in rich and poor nations. As a disease without borders, it exposed how rapidly health system capacity can be overwhelmed, resulting in massive loss of lives and how vaccine access and equitable distribution may contribute to a reverse in pandemic deleterious outcomes, while communities and regions that suffer disproportionate inequitable distribution of available vaccines may be more prone to dismal health outcomes. Contrary to the traditional vaccine development timeline, SARS-CoV-2 disease created a global health emergency that fostered global cooperation in public and private sector and encouraged warp-speed vaccine development through mRNA and viral vector vaccine technology platforms. The success of any medical or public health intervention is predicated on both rapid development of intervention agents and equitable and widespread access. While community pharmacy density was pivotal to vaccine access in the United States, other parts of the developing world can continue to deploy channels already in use for other community disease containment efforts while striving to improve pharmacy density. In the United States, vaccine access through community pharmacies facilitated the pandemic-to-endemic transition, same access; to rapid testing and early treatment would curtail the disease, minimize disease outbreaks, and prevent health system capacity stress. Pharmacists and other health-care professionals should expect larger number of their patients showing up with long-term systemic implications of COVID-19, either as survivors of COVID-19 disease or survivors of relatives lost to COVID-19 disease.
Keywords
COVID-19
Coronavirus
Severe acute respiratory syndrome corona virus-2
Pandemic
Vaccination
Vaccine hesitancy
Point-of-care testing

INTRODUCTION
Some things you never forget! By the first quarter of 2020, I was in the last week of my ambulatory care clinical pharmacy rotation at Spectrum Health in Grand Rapids Michigan, when faculty ordered all students and interns to cease in-person clinical activities immediately and until further notice. Why? The entire world is grappling with COVID-19 disease caused by severe acute respiratory syndrome corona virus-2 (SARS-CoV-2).
SARS-CoV-2 is the world’s seventh disease-causing human coronavirus, after severe acute respiratory syndrome corona virus (SARS-CoV) and Middle East respiratory syndrome coronavirus. SARS-CoV-2 first appeared in late December 2019 causing severe to deadly pneumonia (named COVID-19 disease), characterized by fever, dry cough, dry mouth, loss of taste, difficulty breathing, fatigue, and myalgias. SARS-CoV-2 is both highly contagious and rapidly transmissible. By March 2020, it has spread to 213 countries, prompting a pandemic declaration by the World Health Organization and as of July, has caused over 500,000 fatalities from over 12 million confirmed cases worldwide including over 250,000 US deaths, and by 2021, estimates stand at more than 5 million deaths globally and almost 1 million US deaths.[1] Since that first quarter of 2020 to another first quarter in 2022, vaccination rates have improved, hospitalizations and deaths have declined, and the United States has transitioned from COVID-19 pandemic to an endemic phase. In the United States per the Centers for Disease Control and Prevention (CDC), data from March 2, 2022 indicate 553.8 million vaccine doses given to date out of which at least one dose of vaccine has been received by about 253.8 million people, representing 76.4% of the total United States population, out of which fully vaccinated persons stand at 65% or about 215.8 million.[2]
The fight against SARS-CoV-2 disease is as global as the disease itself, with multifaceted approaches in epidemiological control, prophylaxis by vaccination, monoclonal antibody therapies, and anti-viral pharmacotherapies aimed at alleviating morbidity, shortening length of hospitalization, and reducing mortality. In that global arsenal, vaccines development and deployment remain pivotal, and pharmacists play a critical role, by reason of ready access to the community. In the United States, the pharmacists’ experience as immunization providers in the fight against annual influenza virus represented a natural take-off point as foot soldiers to tackle this new pandemic, and while producing the vaccines in record time was critical, getting enough trained professionals to administer the shots became even more critical. The CDC estimates that there is one community pharmacy within a 5 mile radius of every nine out of 10 Americans, thus positioning the community pharmacist as a natural fit in our fight against the COVID-19 pandemic.[3]
THE SPECTRUM OF CARE IN THE AGE OF COVID-19
Providing care in the age of COVID-19 is a novo responsibility which is both exciting and challenging for community pharmacists and our role kept evolving almost as rapidly as the disease, necessitating an increasing need for pharmacists to update their knowledge about the disease, its course, preventative and treatment options, and an ever-changing public health policy to provide trusted and usable information to their patients. Community access to point of care testing for rapid identification of SARS-CoV-2 infection has been identified as a critical piece for disease containment, and track and trace approach to minimize viral transmission rates to free up health system capacity for more severe cases. To facilitate testing access, the Center for Medicare and Medicaid Services (CMS) allows pharmacies to offer Clinical Laboratory Improvement Amendments (CLIA)-waived COVID-19 laboratory tests by an approved form CMS-116.[4] In our experience, the role requires pharmacists to accurately interpret and communicate results to patients and play the counselor or comforter-in-chief, especially when needing to break news of a SARS-CoV-2-positive test result.
An immediate sequelae of SARS-CoV-2 disease is a greater clinical pharmacy emphasis in the community, in areas of collaborative practice, health maintenance, and prevention as well as transitions of care services, representing a shift from an erstwhile less engaged practice model. Pharmacists who are not expanding into clinical service may soon be losing patronage and revenues.
With COVID-19, there are many questions than answers. The community pharmacist is only a phone call away and that accessibility translates to unprecedented high call volumes in the pharmacy, with pharmacists providing education and counseling to provide assurance, relieve anxiety, or recommend next level clinical intervention.[5] This development, in turn, stresses pharmacy staff and promotes burn-out. Bear in mind too, the pharmacist charges no fees for consultation, and provider status is still a tussle in many states. From the perspective of the community pharmacist, this paper will focus on experiences from the trenches, the impact of the COVID-19 disease on community pharmacy practice model, patient encounters and expectations, vaccine hesitancy and vaccine acceptance, vaccine adverse events, laboratory testing, new opportunities, and a medium to long-term outlook for the profession.
VACCINE ADMINISTRATION WORKFLOW DESIGN
To address this increasing workload, pharmacies devised coping mechanisms with the use of technology, calendar and scheduling tools, and workflow designs. Some online appointment booking software like JotForm have free and paid versions, while others are through paid subscription only. Most formats would allow the pharmacist to designate specific appointment windows driven by staff availability to optimize patient encounters for vaccination. Since patients are already comfortable utilizing appointment model with their doctors’ office, doing the same at the pharmacy is a nobrainer. Diverting pressure away from the typical pharmacy workflow allows pharmacy staff to perform regular pharmacy operations of script filling, medication reviews, clinical consult in person or by phone, and engagement with other professionals in health-care delivery.
Quite unlike regular prescription filling patient encounters at the pharmacy, vaccine administration requires intense patient communication, counseling before, during and after administration, extensive paperwork for documentation, patient monitoring, and documentation of vaccine administration in government registry. When patients arrive at the pharmacy either by appointment or walk-in, pharmacies have had to design a workflow experience to accommodate those vaccine-specific nuances thus de-escalating an already stressful encounter. It is good practice to have a designated vaccination station or miniclinic area for patient privacy and to reduce vaccine administration errors. Practical considerations sometime require vaccine administration at curbside or in the parking lot inside the patient’s vehicle. One component of the workflow design with a high comfort index was the use of digital timers handed to each patient post-vaccination. This sets clear patient’s expectation for their departure time, eliminating questions like; (is it time yet?) and allowing pharmacy staff to concentrate on other ancillary activities. Checking up on patients’ welfare the day after vaccination or at most 3 days after, proved to be a welcome, unexpected, and comforting experience for most patients (COVID-19 VACCINATION PROCESS WORKFLOW in box).
COVID-19 VACCINATION PROCESS WORKFLOW
VACCINE HESITANCY IN THE AGE OF COVID-19
Vaccine hesitancy has always coexisted with vaccines and widespread community resistance to vaccination on grounds of safety and other concerns drove the 1905 Supreme Court ruling on Jacobson v. Massachusetts.[6] Vaccine hesitancy became more prominent due to COVID-19 disease with perceived loss of independence of regulatory agencies eroding public confidence in evidence-based recommendation.
Discussions with individuals about vaccine hesitancy, vaccine acceptance, or vaccine refusal require empathy, non-judgment, and tactful communication based on citable scientific and sometimes anecdotal evidence. The C.A.S.E method – Corroborate, About Me, Science, and Explain/ Advise – offers a promising method to address vaccine hesitancy in the clinic [Figure 1].[7] At the community level, individuals enquire multiple times about vaccination, make, and miss appointments, while some eventually show up at the pharmacy; still expressing hesitancy even at the point of vaccine administration, often citing work or professional requirement for eventual decision to vaccinate. For COVID-19, there is no shortage of references in lay press and professional publications in favor of vaccine safety and efficacy, yet, our experience reveals some individuals change their minds to get vaccinated while some remain yet to be persuaded despite best efforts, and of note; we have had patients asking to be issued the CDC vaccination card without having received any vaccine, to which of course we tactfully decline.

- The C.A.S.E method to facilitate discussions of vaccine hesitancy. Adapted from. Jacobson RM, et al. Vaccine Hesitancy. Mayo Clin Proc. 2015;90(11):1562-1568.
With children ages 5–11 years old + and young adults 12–16 years old, parental engagement and consent are a requirement to obtain vaccines in the US. Our experience even with members of church community where we hold weekly vaccination clinics, show that children from vaccine-hesitant homes were less likely to be vaccinated compared with their peers in more vaccine-receptive households, standing to reason that if a mother is yet to be vaccinated [Figure 2], it could be social dissonance to bring in the kids for shots that mothers themselves would not accept. Jacobson et al. (2015) stated that clinicians struggle with parental vaccine hesitancy, and in a 2015 study, clinicians report that parents routinely request delaying vaccines and that clinicians routinely acquiesce.[7] Realizing then that vaccine delay/procrastination is a sequelae of vaccine hesitancy, we deconstructed the time required to achieve immunity; using Pfizer SARS-CoV-2 vaccine scheduling to sound a wakeup alarm and mitigate the procrastination component of vaccine hesitancy. It was a light-bulb moment with message targeted at providers and doctors’ offices, YMCA, Gyms, Football Clubs, etc., people who have contact with vaccine hesitant parents. Our message is built around the SBAR communication model, with immediate appeal to health professionals but also explained in a way understandable by the non-professional audience. The message is simple: Individuals require 35 DAYS for immunity to approach FULLNESS when administered the Pfizer COVID-19 vaccine (Dose 1 at Day 0, Dose 2 at Day 21, and 14 days after dose 2, patients approach 100% immunity. 0 + 21+ 14 = 35, which is = 5 WEEKS).[8] This approach is corroborated by Goldstein et al. in health communication and vaccine hesitancy, where incorporating an appropriate selection of available communication tools forms an integral part of every immunization program to address specific factors driving hesitancy in any target population.[6,9]
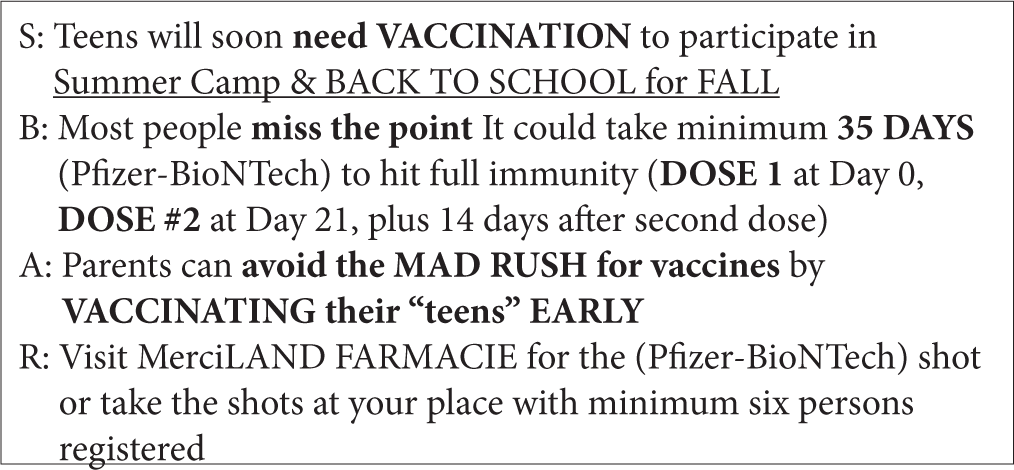
- SBAR tool adaptation by MerciLAND FARMACIE to address vaccine hesitancy among teenagers
COVID-19 IMPACT ON VACCINATION RATES OF OTHER VACCINES
One of the earliest uncertainties surrounding COVID-19 vaccination was the fear of numerous unknowns not so much in terms of efficacy but rather the safety or otherwise of COVID-19 vaccines. Clinical rotation at BV Drug, Buena Vista, and Colorado provided access to a convenient sample of respondents to gauge the impact of COVID-19 on vaccination rates of other vaccines. BV drug has a large immunization program, administering approx. 2000 flu shots in 2019, both from pharmacy walk-ins and offsite flu clinics, for 2020; due to COVID-19 as confounder for other disease states including COPD, asthma, diabetes, and immune disorders, a 20–30% increase in immunization rate was projected, and it was hypothesized that COVID-19 will lower vaccine hesitancy and cause an uptick in adoption rates of other vaccines across populations. The pharmacy promotes FLU IMMUNIZATION as the entry point and introduces other vaccines to appropriate patients on contact.
Our approach was to orally question a convenient sample of regular flu vaccine recipients in a 3–5 min conversation in-person or by telephone for their receptivity to COVID-19 vaccination [Figure 3].

- Response from convenient sample of likely recipients of influenza and COVID-19 vaccines.
OTHER PATIENT ENCOUNTERS
As clearer pictures emerge on the devastating impact of COVID-19, especially on vulnerable patient populations with comorbidities, at another community pharmacy, MerciLAND FARMACIE in Southgate Michigan, between October and December 2021, individuals 65 years old + were more receptive to FLU vaccination as they receive their COVID-19 shots. It was a much easier sell as the CDC encourages practitioners to utilize every patient encounter for vaccine rate optimization. With persons 50 years old and above, the encounter represents opportunity for patient education on vaccine-preventable pain of post-herpetic neuralgia from herpes zoster virus infection which occurs in one out of every three adults 50 years old and above and which is preventable by shingles vaccination.
In the younger population, as they bare their arms for COVID-19 vaccine, the pharmacist has opportunity to notice tattoos and body markings prompting tactful conversations around hepatitis B vaccination, the virus transmissibility through blood or body fluids and stating clearly that persons at risk include health care workers and individuals who may be exposed to possibly contaminated body piercing equipment.[10]
Regardless of the age group, a proven method to optimize the encounter for increased vaccination rate is predicated on the practitioner stating with firmness that a review of patient’s profile or other appropriate assessment indicates that they are due for specific vaccine(s) and they can take the extra shot(s) on their visit today.
VACCINE ADMINISTRATION, DOSE OPTIMIZATION, ERRORS PREVENTION, AND ERROR REPORTING
From the first shot of COVID-19 vaccine, given December 14, 2020, in New York,[11] the overarching strategy was for health-care providers to vaccinate-at-all-costs every willing individual with less emphasis placed on un-usable portions of any punctured vaccine multidose vial, which depending on the manufacturer has different beyond-use expiry times once opened. By the beyond-use expiry window, any un-used portions of the vaccine are discarded, regardless of whether nine doses were used or nine doses remain, for example, in a 10-dose multivial. The strategic aim was to accelerate vaccination rate with an eye toward achieving herd immunity as fast as possible.[12] As infection rates dropped and hospitalizations fell back within capacity of our health-care system, we saw a strategic shift from vaccinate at all costs to optimize vaccine doses, to reduce vaccine wastage. In our community pharmacy practice, we implemented vaccine return/wastage reduction strategies including patient packing through our appointment-based model, where we schedule multiple patients within the beyond-use expiry time of any opened vaccine vial. Furthermore, the beyond-use expiry time of some vaccine products like Janssen COVID-19 is optimized by refrigerating the punctured vial at 2–8°C or 35.6–46.4°Fahrenheit instead of at room temperature thus effectively increasing the beyond-use expiry time from 2 to 6 h.[13]
As results from multiple clinical trials for different patient populations emerge, FDA emergency use authorizations (EUAs) for vaccine products occurred and changed rapidly, with a deluge of product information for health care workers and an attendant probability for vaccine administration errors. According to the Institute for Safe Medication Practices (ISMP), errors reported included dilution errors in vaccine mixing, administration of vaccines past their beyond-use time, dosing error, vaccine administration to patients outside the recommended age ranges, and others. We also employed the teach-back method allowing the patient to sight their vaccine prior drawing into the syringe and confirming aloud the name of the vaccine and age range, every shot, every time; a method later validated by ISMP to reduce vaccine administration error.[14] To further minimize error potential, we implemented error prevention strategies utilizing enhanced pharmacy processing software stops to verify vaccine appropriateness for patient age, the right dose for every vaccine and dosing interval for vaccines requiring two-dose series and lately, booster shots. To forestall dosage administration errors on the booster dosing for the Moderna vaccine, we posted current important FDA prescribing information for vaccination providers[15] at drop-off, pharmacist verification bay, and vaccine administration areas representing strategic contact points in the vaccine prescription processing workflow. In addition, we sounded alarm on booster booby traps to pharmacy staff and professional colleagues through our LinkedIn platform.[16] In one event where vaccines were administered past their beyond-use time range, contact with the manufacturer confirmed acceptable vaccine stability and viability for safety and efficacy and despite any report or knowledge of any patient adverse event, the incident was still reported as required into the CDC’s vaccine administration error reporting system (VAERS).[17]
COVID-19 TESTING IN COMMUNITY PHARMACY
Fighting the COVID-19 pandemic required multipronged epidemiological and pharmacotherapeutic approaches toward prevention, intervention, palliative, and treatment. Reducing the rates of viral transmission, disease progression, and hospitalizations depend on timely detection of infection which, in turn, impacts implementation of quarantine and isolation guidelines. The effectiveness of the testing component, therefore, depends on easy accessibility to tests in symptomatic and asymptomatic individuals who possibly had contacts with infected persons. Since patients already access community pharmacies for their COVID-19 vaccines, it was a natural service extension for patients to receive their COVID-19 tests in the same neighborhood pharmacy. The CMS grants CLIA-waiver certification for community pharmacies to offer pharmacist-administered COVID-19 rapid antigen testing and COVID-19 antibody testing. In another model, pharmacies enter into collaborative practice agreement with approved laboratories and act as sample collection centers for placement in biohazard drop boxes located outside of their pharmacies for subsequent collection for analysis at a remote laboratory. In other variations of the model, pharmacies simply act as pipeline providing test kits to patients who self-collect their samples at home and either ship out the kit using the prepaid package or return it to the nearest collaborating pharmacy. Pharmacies are also seeing more of their patrons requesting elective COVID-19 tests before hospital procedures. The travel and tourism industry also continue to require proof of negative laboratory-based PCR COVID-19 test results as a condition of service to potential customers. MerciLAND FARMACIE retained practice agreements with local laboratory, Noor Diagnostics in Dearborn Michigan and more recently with eTrueNorth,[18] a National Laboratory COVID-19 Free Testing platform sponsored by the United States Department of Health and Human Services through our collaborative practice agreement facilitated by Prescribe Wellness. Regardless of the model, pharmacists who provide the channel and professional supervision are finding that the opportunity is professionally satisfying and represents additional revenue source in an industry smirking under the weight of its own share of pandemic-imposed economic burden.[19]
VACCINE DEVELOPMENT MEASURES AND DELIVERY
Containing a rapidly transmissible SARS-CoV-2 global pandemic required an equally rapid response from multiple angles, most critical of which is vaccine development. While traditional vaccine development could take 5–10 years to accumulate safety and efficacy data from animal studies through Phases 1–3 clinical trials and time-dependent regulatory approval processes,[20] a bright spot in our global fight against SARS-CoV-2 was the ready availability of subjects for clinical trials. Add to that was the urgency and willingness to collapse multiple steps of the trial phases, readiness of regulatory bodies to grant emergency use authorizations following initial demonstration of safety and at least 50% efficacy of candidate vaccines,[21] preemptory financial investment of the private sector in vaccine manufacturing at scale. Pre-clinical and clinical trial research reports on dozens of mRNA vaccines in treating cancer, viral diseases, and non-targeted gene diseases confirm the reliability and effectiveness of the mRNA vaccine technology platform resulting in rapid deployment toward the development of vaccines against SARS-CoV-2 disease. For instance, compared to the typical vaccine 5–10 years for traditional vaccine development, the National Institute for Allergy and Infectious Disease and Moderna Pharmaceuticals jointly developed the world’s first COVID-19 vaccine mRNA1273 to undergo clinical trial in a mere 63 days from SARS-CoV-2 genome sequence release to clinical Phase 1, underlying the potential for rapid and more robust response to any emerging disease or even another pandemic.[22]
The success of any medical or public health intervention is predicated on both rapid development of intervention agents and equitable and widespread access. While community pharmacy density was pivotal to vaccine access in the United States, other parts of the developing world can continue to deploy channels already in use for other community disease containment efforts while striving to improve pharmacy density. The CARAMAL study for instance in the distribution of rectal artesunate against malaria, in the Democratic Republic of Congo, Nigeria and Uganda, utilized Community Health Workers, and Primary Healthcare Centers due to their easy access to villagers who are cutoff from other formal public health providers.[23]
FUTURE OUTLOOK
Although the world is gradually accessing a COVID-19 disease pandemic to endemic transition, sustainable containment of the disease like the annual influenza disease would require global vaccine equitable access and a local test-to-treat model, involving early identification of infected individuals and initiation of anti-viral therapy for rapid remission and risk reduction for morbidity and hospitalization. In the United States, since vaccine access through community pharmacies facilitated the pandemic-to-endemic transition, same access; to testing and treatment at the community pharmacy to manage the endemic, especially in the early phase, would curtail the disease, minimize disease outbreaks, and prevent health system capacity stress. In the medium to long term, pharmacists and other health-care professionals should expect larger number of their patients showing up with long-term systemic implications of COVID-19, either as survivors of COVID-19 disease or survivors of relatives lost to COVID-19 disease.
Acknowledgments
Author expresses appreciation to BV Drug in Colorado and their principals Dr. Lucas Smith PharmD and Dr. Lauren Gover PharmD; preceptors for my clinical rotation in their disease state management/community clinical pharmacy practice in partial fulfilment of requirement for my PharmD with the Skaggs School of Pharmacy, Colorado 2020.
Author also thanks Olugbenga Siyanbola, BPharm, RPh, Staff Pharmacist, MerciLAND FARMACIE for collaborative work in the development and application of the COVID-19 Vaccine Process Workflow. Much thanks also go to Dr. Okezie I. Aruoma for his well-considered encouragement on this project and finally, special thanks to Grace Bolanle, VP Operations, MerciLAND FARMACIE for administrative support and nursing roles during our mass vaccination clinic.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Olugbade O. Bolanle is an Associate Editor of the journal.
References
- The outbreak of the novel severe acute respiratory syndrome corona virus 2 (SARS-CoV-2): A review of the current global status. J Infect Public Health. 2020;13:1601-10.
- [CrossRef] [PubMed] [Google Scholar]
- Covid Tracker Weekly Review. Atlanta, Georgia: Centers for Disease Control and Prevention; Available from: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html [Last accessed on 2022 Jul 03]
- [Google Scholar]
- Community pharmacists' contributions to disease management during the COVID-19 pandemic. Prev Chronic Dis. 2020;17:200317.
- [CrossRef] [PubMed] [Google Scholar]
- Centers for Medicare and Medicaid Services. Clinical Laboratory Improvement Amendments (CLIA).
- [Google Scholar]
- Community pharmacists roles during the COVID-19 pandemic. J Pharm Pract 2020
- [CrossRef] [PubMed] [Google Scholar]
- Vaccine confidence in the time of COVID-19. Eur J Epidemiol. 2020;35:325-30.
- [CrossRef] [PubMed] [Google Scholar]
- LinkedIn Article: (June 2021) Addressing Vaccine Hesitancy: CNN Agrees with Dr. ToSH. Available from: https://www.linkedin.com/pulse/cnn-agrees-dr-tosh-tosh-bolanlepharmd-mba-rph [Last accessed on 2022 Jan 03]
- [Google Scholar]
- Health communication and vaccine hesitancy. Vaccine. 2015;33:4212-4.
- [CrossRef] [PubMed] [Google Scholar]
- Hepatitis B Questions and Answers for Health Professionals. Atlanta, Georgia: Centers for Disease Control and Prevention; 2022.
- [Google Scholar]
- State strategies for addressing barriers during the early us COVID-19 vaccination Campaign. Am J Public Health. 2021;111:1073-77.
- [CrossRef] [PubMed] [Google Scholar]
- Dynamics of Population Immunity Due to the Herd Effect in the COVID-19 Pandemic. Vaccines (Basel). 2020;8:236.
- [CrossRef] [PubMed] [Google Scholar]
- Janssen COVID-19 Vaccine EUA Fact Sheet for Healthcare Providers Administering Vaccine.
- [Google Scholar]
- Available from: https://www.ismp.org/alerts/mix-ups-between-influenza-flu-vaccine-and-covid-19-vaccines [Last accessed 2022 Feb 28]
- Moderna Fact Sheet. Available from: https://www.Users/Pharmacy/Desktop/VACCINES/MODERNA/eua-fact-sheet-providers.pdf [Last accessed on 2021 Oct 15]
- [Google Scholar]
- Linkedin Article. Addressing Vaccine Dosing Error: Booster Booby Trap. 2021. Available from: https://www.linkedin.com/posts/activity-6857003834556981248-HpR6 [Last accessed on 2022 Jan 03]
- [Google Scholar]
- Vaers. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/vaers.html [Last accessed on 2022 Jul 03]
- [Google Scholar]
- Covid-19 Testing Platform. Available from: https://scrnc5.pdhi.com/CXClient/FindVoucher.aspx?__XXX=X0NvbnRleHQ9NDkyOTYxMDglM2E0MTUlM2E2ODglM2EyODI1JTNhMTM0NCUzYSUzYU4%3d [Last accessed on 2022 Mar 07]
- [Google Scholar]
- (APhA) Pharmacy Models for COVID-19 Testing Washington, DC: American Pharmacists Association; 2022.
- [Google Scholar]
- Development and delivery systems of mRNA vaccines. Front Bioeng Biotechnol. 2021;9:718753.
- [CrossRef] [PubMed] [Google Scholar]
- Licensure and Emergency use Authorization of Vaccines to Prevent Covid-19: Clinical Considerations In: Vaccines and Related Biological Products Advisory Committee. 2020.
- [Google Scholar]




